“The Hidden Disease”:
The Overlooked Economic Impacts of Endometriosis
By: Leah Moody, BBA, MBA

Dr. Linda Griffith is one of the best bioengineers in the world. She was instrumental in developing the process of growing human body parts on the backs of white mice. During her journey to becoming a world-class scientist, Dr. Griffith suffered through horrible pain for many years. All of her doctors told her the incredible pain she felt was just part of being a woman. An emergency surgery at age 27 finally revealed the truth, Dr. Griffith suffers from endometriosis. After a distinguished career in biogenetics, Dr. Griffith has made a pivot to open the first and only lab in the U.S. to study endometriosis since she discovered her niece also has the disease. When Dr. Griffith realized there was no better treatment for her niece today than what she received thirty years ago, the scientist became resigned to bring the matter to the attention of the scientific community. “It is no longer a woman’s issue,” says Dr. Griffith, “I am making it an M.I.T. issue (Gross).”
The oldest and most common disease in women is still one of the biggest mysteries of modern medicine. No one knows what causes it. There is no treatment, no test for diagnosis, and no cure. Endometriosis has been around as long as women, yet extraordinarily little attention has been given to this debilitating, painful, and widespread disease (Whelan). Countries with public health insurance have just recently started to take notice of the vast numbers of women who cannot function due to endometriosis. It is widely reported that one in ten women have the disease, but a recent increase in studies is starting to find that the number is actually double what was originally suspected (Facts). To put the situation into perspective, the U.S. currently has only one medical lab and two health clinics dedicated to helping women with endometriosis (Gross). The estimated 33 million U.S. women who suffer from endometriosis are mostly on their own.
What is Endometriosis?
Endometriosis occurs when the lining of the uterus grows outside of the uterus. Most commonly, endometriosis is found on the ovaries, bladder, bowels, and stomach, but it can be found anywhere in the body. Rare cases include the heart, lungs, brain, and spine. Lesions of endometriosis work like glue and fuse organs together when they turn into petrified scar tissue, but first they can cause incredible pain. It is the leading cause of infertility and pelvic pain in women (Facts). There are literally dozens of symptoms of endometriosis, although most of them are not unique to the disease. The hot flashes, nausea, bloating, fatigue, and severe pelvic pain are usually written off as natural side effects of having a “bad period” or “hormonal problems.” Endometriosis pain can occur at any time without warning and often leads to trips to the emergency room and long periods of bed rest. Misdiagnosis occurs because endometriosis cannot be seen with radiology or blood tests. A diagnosis of endometriosis can only be officially confirmed from laparoscopic surgery and even then, the doctor must be looking for it with a microscope to find it (Whelan). The average diagnosis takes 7.5 years, but most women go without a diagnosis at all (Wise). Endometrium tissue is the most regenerative tissue found in humans. More than 85 percent of the time, after endometrial lesions are removed through surgery, they grow back (Siman). More than 70 percent of women who have endometriosis surgery repeat the procedure, often multiple times (De Graaf). Dr. Linda Griffith has had the surgery eight times and never gained any respite from the pain (Gross). Each surgery leaves more scar tissue, which causes a longer recovery time, and can interfere with the function of organs such as the bladder, bowels, ovaries, and stomach. The scar tissue left from the surgery is said to cause as many problems as the disease itself.
The pain of endometriosis often causes women to miss work and school. Because the disease is so misunderstood in the U.S., surgery is considered elective. Many insurance companies categorize it as a disease of infertility and therefore do not cover any of the medical expenses associated with endometriosis. There is no treatment available for low-income women. The significant impacts of endometriosis are not just physical and emotional, but financial.
Problems in Studying the Financial Costs Associated with Endometriosis
Endometriosis is called “the hidden disease” not just because it is invisible to the naked eye, but because the illness and its life-changing impacts have historically been ignored worldwide. Congresswoman Abby Finkenauer was the first person to say the word “endometriosis” on the floor of U.S. House of Representatives in 2016. Her personal journey led her on a mission to secure funding for endometriosis research. Finkenauer successfully lobbied to double government sponsored funding from $13 million to $26 million that same year (“Abby”). Most of the funds were earmarked for The Center for Gynepathology Research run by Dr. Griffith because it is the only laboratory dedicated to endometriosis in the U.S. (Gross). Finkenauer lost re-election in 2020 and endometriosis warriors lost their only champion in Congress. There is no current plan to make future funding a public priority in the U.S.
There are three well-known studies created in the U.S. to study the financial costs associated with endometriosis from 2005-2012. All of them highlighted the concern that economic impacts of the disease were substantial and ignored (Simoens S, Dunselman). According to the American Society for Reproductive Medicine, “Health economic information for endometriosis is scarce, limiting our understanding of its overall economic impact (Gao).”
In 2010, the World Endometriosis Research Foundation (WERF) started a regular study on the economic impacts of endometriosis. The “EndoCost Study” includes ten countries and aims to find the cost drivers and socio-economic impacts of endometriosis around the world Simeons S, Dunselman). WERF is the only international organization known to formally study the direct and indirect financial impacts of endometriosis. The funding for WERF comes from private donations and is not supported by any government.
The results of the WERF study validate the hypothesis that the lack of productivity and quality of life issues caused by endometriosis noticeably affect not just the woman who suffer from the disease, but by society as a whole. The EndoCost study includes data from 13 centers that specialize in endometriosis care. Each center has an economist with a vested interest in studying the fiscal effects of the illness. Problems with the study include a difference in measuring the costs in the U.K. and the Netherlands against all the other countries. The U.K. and the Netherlands actually base medical prices on costs, whereas economists in countries such as Germany and the U.S. base costs on price sheets. Also, productivity was measured against national averages of weekly salaries instead of the actual salaries of the observation sample. When there was no national index available, the current U.K. salary index is used and then adjusted for expected mortality. (Simoens S, Dunselman).
Indirect Costs
The WERF study finds that 66 percent of financial losses for the women who have endometriosis are due to loss of productivity (Simoens S, Dunselman). Long recoveries from surgeries, doctors visits, and sick days due to acute symptoms are indirect costs that cause time away from work, school, and other income drivers. Almost a third of patients reported problems with usual activities. More than 16 percent of women studied report problems with mobility. Fifty-six percent of endometriosis suffers report problems with depression and anxiety. Two of the women in the WERF study consider their current state of health worse than death (Simeons S, Dunselman). Endometriosis support groups use Facebook and other forums to honor members who have committed suicide. Currently, there is no national or international tally of suicides caused by endometriosis, however evidence suggests that those cases exist in each country studied (Whelan).
Another major financial effect from endometriosis that is hidden in plain sight is from divorce. Endometriosis is a leading cause of divorce for the women who suffer from endometriosis in all ten of the countries in the study by WERF (Simoens S, Dunselman). Chronic illness puts a heavy strain on familial relationships. Women who suffer from endometriosis often need physical assistance at home and can be a burden to their partners both physically and financially (De Graaf).
None of the major studies on the economic impacts of endometriosis include the cost of fertility treatments for the tens of millions of women worldwide who are infertile from the disease (Soliman). It has long been known that endometriosis is the number one cause of infertility in women. Invitro fertilization, egg freezing, hormone treatments, surgeries, and other methods of treating infertility can cost a fortune. According to the NIH, the average cost for a successful series of fertility treatments in the U.S. is $61,377 (Katz). The costs are not officially counted as being associated with the financial impacts of endometriosis, though it is the most common cause for them.
Direct Costs
The largest direct medical cost for endometriosis is surgery. There is a significant shortage of surgeons who can perform the surgery safely because it involves removing lesions and scar tissue across multiple organs. Performing a surgery on bowels is risky, difficult, and takes special skill and experience (Rogers). Most regular gynecologists in the U.S. refer patients to infertility specialists for treatment. Because endometriosis is the leading cause of infertility, these specialists are the most experienced experts available to perform the complicated surgeries needed. In the U.S., insurance companies do not usually cover the cost of infertility specialists because issues dealing with infertility are considered elective. Doctors who specialize in infertility measure their success on the ability to help their patients have a successful pregnancy. Therefore, women who have endometriosis pain but do not wish to have a baby are turned away from these doctors more than 90 percent of the time (Whelan). Studies on the cost of endometriosis surgeries are riddled with limitations because each doctor charges whatever they want in the U.S. Prices range from $20,000 to $150,000 depending on the specialist, the type of surgery performed, and the subsequent recovery (Siemens S, Dunselman). Around 25 percent of women who have an endometriosis surgery do not seek another procedure either because they gained relief or because the pain caused by the surgery was too much to repeat. Around 65 percent of women have an average of three surgeries in an effort to lesson the physical pain. Ten percent of women who seek surgery repeat the procedure four or more times (Facts). In the event that an insured woman can find a gynecologist to perform the surgery, across the entire U.S., doctors require a down payment equivalent to the out-of-pocket maximum of their policies before they will book a surgery date. Gynecological surgeons then bill the insurance company for the surgery naming problems like pelvic inflammatory disease, polycystic ovarian syndrome, and cyst removal without ever mentioning any diagnosis of endometriosis because most policies will not cover it (Rogers). The current policies put the greatest financial burden on the woman, so only those who have thousands of dollars available for the out-of-pocket expenses receive any help in the U.S. Women often use their savings, including retirement savings, to pay for the surgery (Wise). Current policies are also prohibiting the scientific community from obtaining any meaningful data about the cost of endometriosis surgeries because they are not recorded as such. Surgeries provide an albeit temporary relief to most women, allowing them to go back to work for a time. Therefore, leaving low-income and uninsured women untreated creates a greater loss of productivity to the women and society.
The second largest direct cost of endometriosis is consultations with specialists. Diagnosis takes an average of 7.5 years because a woman who experiences endometriosis pain and inflammation for the first time usually has no idea where to start (Gao). Bladder specialists usually lack a general knowledge of endometriosis, although bladder pain and misfunction is one of the most commons symptoms of the disease. A woman looking for a diagnosis from a bladder specialist is usually turned away without help because endometriosis in invisible to radiological and other tests (Wise). The same woman will visit multiple specialists looking for the source of the pain. Gynecologists, gastroenterologists, urologists, endocrinologists, oncologists, internal medicine, and pain management doctors are all common stops on the journey to diagnosis and all will yield the same result, inconclusive but expensive tests. Copayments, appointment fees, blood tests and tests like sonograms, MRIs, and CT scans are costs associated with each stop at a specialist (Simoens S, Hummelshoj).
The third largest direct cost of endometriosis is prescription drugs. Because there has never been an official drug therapy created to treat endometriosis, women are forced to take a myriad of drugs to deal with each symptom separately (Siemens S, Dunselman). Since most women have not received an actual diagnosis of endometriosis, attacking individual symptoms is the only strategy available (Rogers). Hormones are at the center of long-term approaches. Every woman has a unique make-up of hormones and can spend years trying different combinations of drugs looking for relief (Facts). Pain killers are an absolute must for women who experience severe symptoms and should also be factored into the costs of treatment (Whelan). Steroids, nonsteroidal anti-inflammatories, drugs for nausea and other digestive issues, blood thinners, anti-depressants, and migraine medicines are all used in an effort to curb symptoms of endometriosis (Rogers).
Other direct expenses include homeopathic and over-the-counter treatments such as special foods, vitamins, laxatives, physical therapy, yoga classes, heating pads, tens units, and special bedding (Soliman). There are dozens of books published by women who have endometriosis giving recommendations of different combinations of these things that have worked for them. Companies who make special vitamins or extracts make a lot of money offering their product or special diet as a “cure to endometriosis (Whelan).”
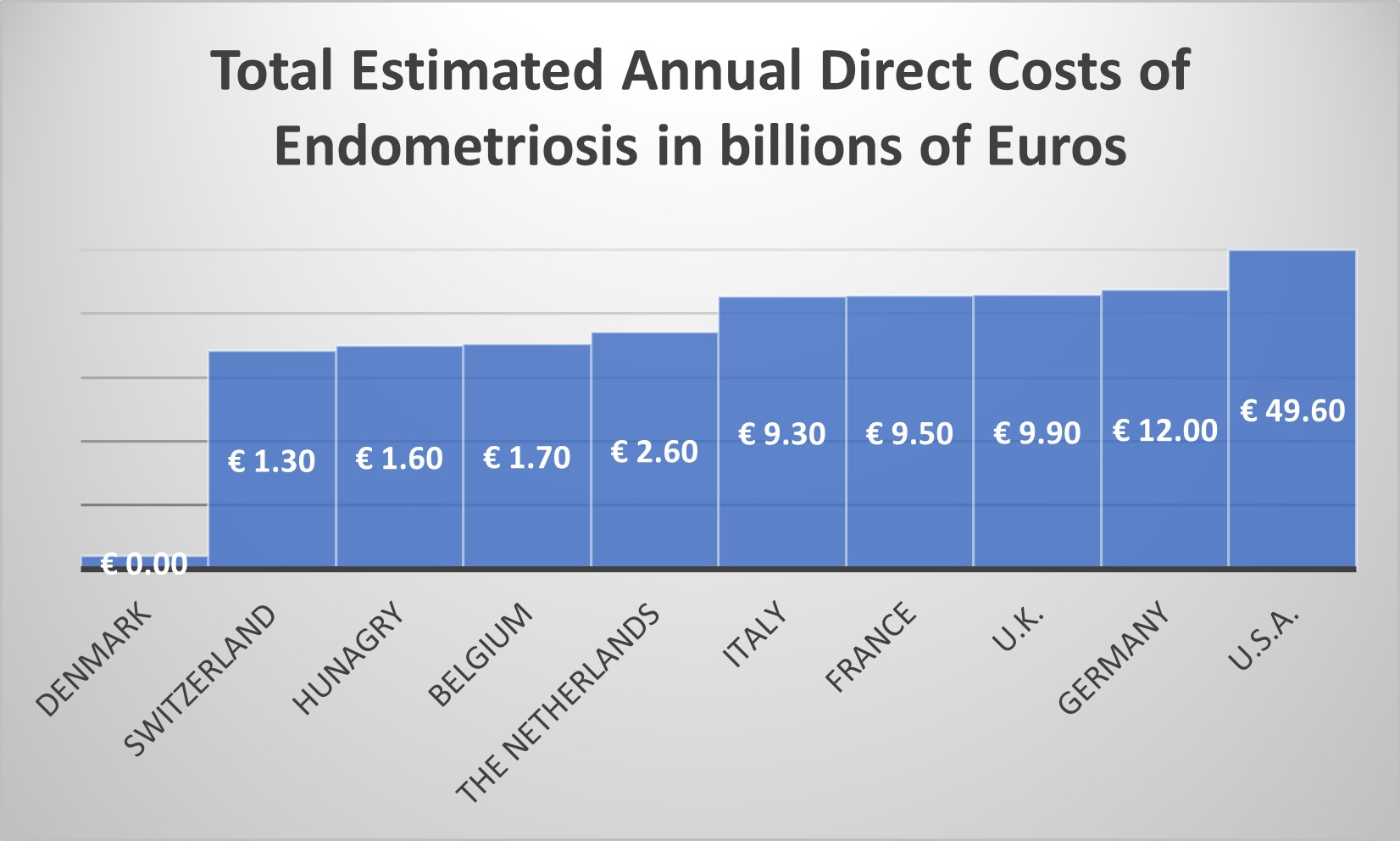
The WERF study results are highly theoretical due to the complicated and limited nature of information related to endometriosis. Of the ten countries who participated, Denmark reported the lowest direct costs at around €800 million while the largest costs were reported in the U.S. at an estimated €49.6 billion. The table below lists participating countries and their estimated costs based on the WERF study (Siemens S, Dunselman):
The authors of the WERF study admit they either overestimated costs because only the most serious cases are reported or underestimated because of a lack of diagnosis and recorded data (Siemens S, Dunselman). The study concludes that the costs associated with endometriosis are about the same as other chronic diseases such as Chron’s Disease and arthritis. The main thesis of the study is that the costs of endometriosis of currently incalculable because of the lack of research available and the vast number of women believed to suffer from the disease without any diagnosis.
Conclusion
Endometriosis is a chronic and painful disease that affects the quality of life of more than 80 percent of the women who are diagnosed with it. While reports vary between 10 and 20 percent of all women having the disease, less than a third of those will receive a diagnosis during their life. Society suffers an economic loss from literally over an estimated hundred million worldwide being kept from having a quality of life that allows them to work or participate fully in their communities. Women have a direct financial burden, especially in the U.S., because private insurance companies do not often cover the cost of endometriosis surgeries and other treatments.
Because the word “uterus” remains tabu in most societies, there are no civic discussions surrounding the public health crisis happening from endometriosis. Countries that carry public health insurance are the main source of data because care and diagnosis is much more likely in those nations. There is no country in the world that has made the study and treatment of endometriosis a top priority. According to Dr. Griffith, the reason for this is most medical researchers are men. Lack of research and political will to solve the problem translates into no viable studies that comprehensively look the economic impact of endometriosis. All reported estimates are highly theoretical and do not carry empirical results that can be verified.
References
“Abby Finkenauer, Congresswoman.” Endometriosis: Causes - Symptoms – Diagnosis
and Treatment, Endometriosis.org, 2021, www.endofound.org/-/abby-finkenauer.
De Graaff AA, D'Hooghe TM, Dunselman GA, Dirksen CD, Hummelshoj L; WERF
EndoCost Consortium, Simoens S. The significant effect of endometriosis on physical, mental, and social wellbeing: results from an international cross-sectional survey. Hum Reprod. 2013 Oct;28(10):2677-85. doi: 10.1093/humrep/det284. Epub 2013 Jul 11. PMID: 23847114.
Gao X, Outley J, Botteman M, Spalding J, Simon JA, Pashos CL. Economic burden of
endometriosis. Fertil Steril. 2006 Dec;86(6):1561-72. doi: 10.1016/j.fertnstert.2006.06.015. Epub 2006 Oct 23. PMID: 17056043.
Gross, Rachel E. “They Call It a 'Women's Disease.' She Wants to Redefine It.”
NYT.com, The New York Times, 27 Apr. 2021, www.nytimes.com/2021/04/27/health/endometriosis-griffith-uterus.html.
Rogers PA, D'Hooghe TM, Fazleabas A, Gargett CE, Giudice LC, Montgomery GW,
Rombauts L, Salamonsen LA, Zondervan KT. Priorities for endometriosis research: recommendations from an international consensus workshop. Reprod Sci. 2009 Apr;16(4):335-46. doi: 10.1177/1933719108330568. Epub 2009 Feb 5. PMID: 19196878; PMCID: PMC3682634.
Simoens S, Dunselman G, Dirksen C, Hummelshoj L, Bokor A, Brandes I, Brodszky V,
Canis M, Colombo GL, DeLeire T, Falcone T, Graham B, Halis G, Horne A, Kanj O, Kjer JJ, Kristensen J, Lebovic D, Mueller M, Vigano P, Wullschleger M, D'Hooghe T. The burden of endometriosis: costs and quality of life of women with endometriosis and treated in referral centres. Hum Reprod. 2012 May;27(5):1292-9. doi: 10.1093/humrep/des073. Epub 2012 Mar 14. Erratum in: Hum Reprod. 2014 Sep
Simoens S, Hummelshoj L, D'Hooghe T. Endometriosis: cost estimates and
methodological perspective. Hum Reprod Update. 2007 Jul-Aug;13(4):395-404. doi: 10.1093/humupd/dmm010. PMID: 17584822.;29(9):2073. PMID: 22422778.
Soliman, Ahmed M., et al. "Incremental direct and indirect cost burden attributed to
endometriosis surgeries in the United States." Fertility and sterility 107.5 (2017): 1181-1190.
Whelan, Emma. “Putting Pain to Paper: Endometriosis and the Documentation of
Suffering.” Health, vol. 7, no. 4, 2003, pp. 463–482. JSTOR, www.jstor.org/stable/26649592. Accessed 20 June 2021.
Wise, Jacqui. “NICE Urges GPs to Diagnoses Endometriosis More Quickly.” BMJ:
British Medical Journal, vol. 358, 2017. JSTOR, www.jstor.org/stable/26940976. Accessed 15 June 2021.